Curating Evidence¶
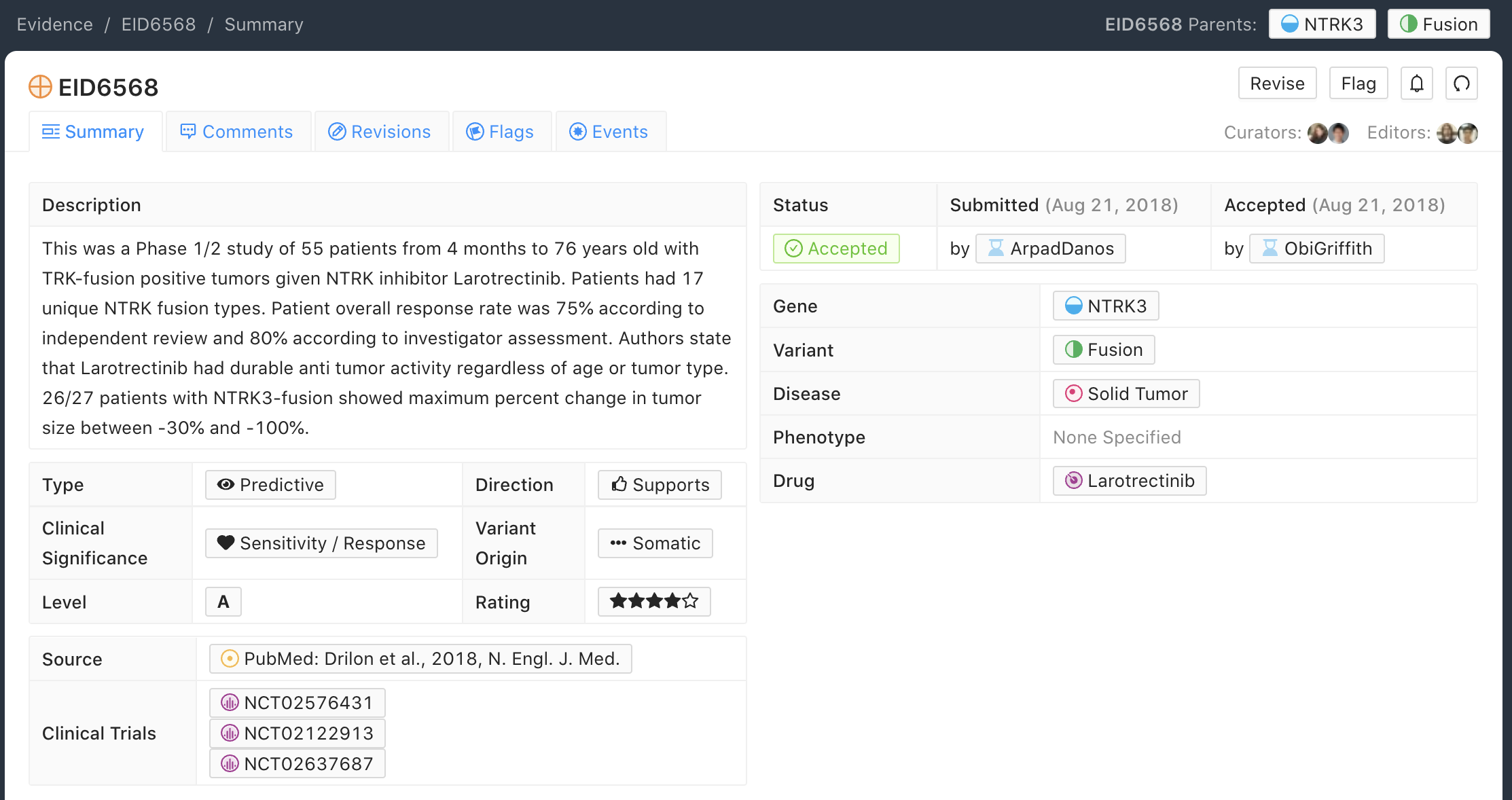
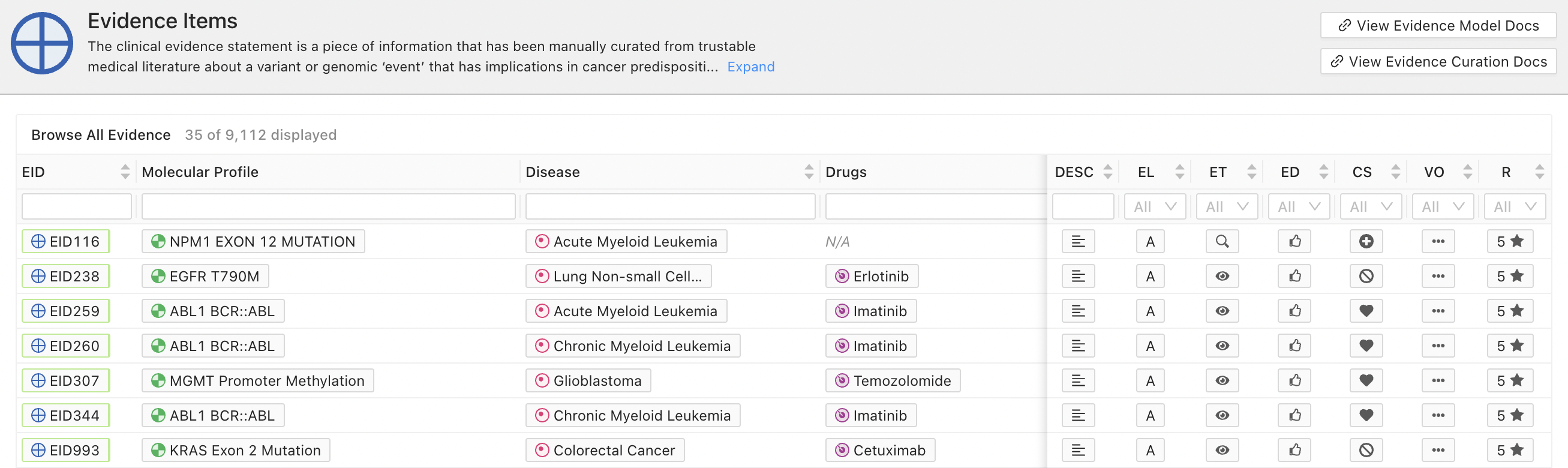
Evidence Items (EIDs) are the fundamental unit of the CIViC knowledgebase. EIDs derive structured clinical statements from peer reviewed, PubMed-indexed publications and American Society of Clinical Oncology (ASCO) or American Society of Hematology (ASH) abstracts, which act as primary Sources for Evidence Items. EIDs link back to their sources. EIDs are hand-curated units of knowledge, and one evidence source may supply enough data to create multiple EIDs. EIDs are displayed throughout the CIViC application, for example as a summary (Figure 1) and as a data table row (Figure 3).
CIViC Evidence is added and curated via a moderation process that includes submitting, evaluating, accepting (or rejecting), and suggesting changes (Figure 2). CIViC Curators may add or suggest revisions to curated content at each step. Adding content involves submitting new Evidence Items or Assertions that subsequently undergo revision and Editor review. Revision of content involves adding or revising the clinical summary and/or its associated features. Once changes are made within the CIViC database, the additions/revisions become visible directly or on a separate revision page depending on the type of submission. Curation is listed as a “Submitted” (i.e., pending) until it is accepted by an Editor, who have the power to accept or reject Curator submissions. Curators may reject (but not accept) their own submissions/revisions. This is useful when a curator realizes they have made an error they wish to correct.
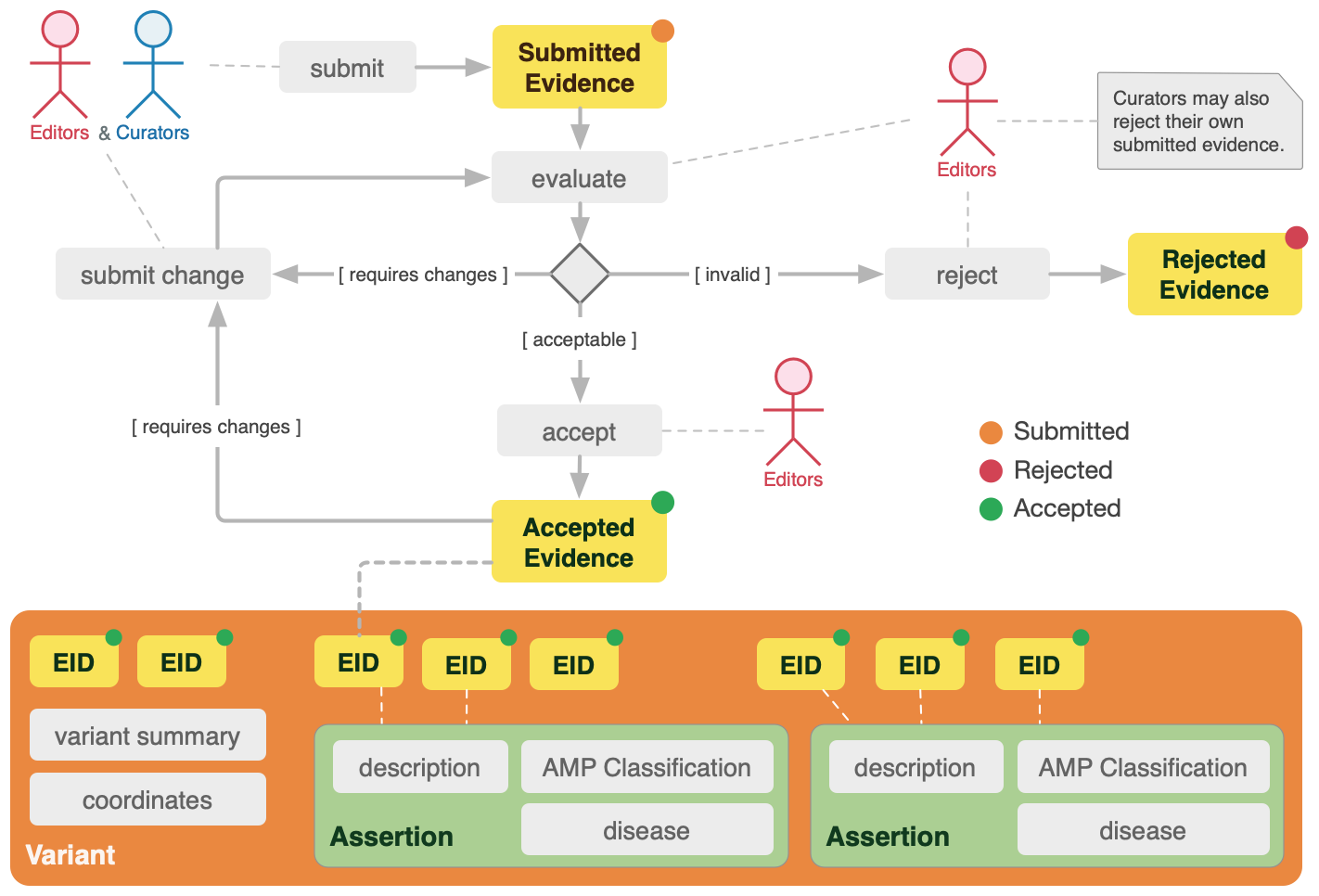
It is important to note that once evidence is submitted into CIViC as a new Evidence Item, then the EID is visible to the community in the unmoderated/non-reviewed state, and these EIDs are labeled in yellow (Figure 3). This enables the public to comment or create moderations on the submitted evidence. It is also important to note that yellow Evidence Items may be incomplete, not accurately fit into the CIViC data model, or contain problems which the moderation process is designed to capture and fix. Once a CIViC EID has been reviewed by editors, and all revisions reviewed and accepted, then the EID is accepted by an editor, and its label changes to green. Mousing over an EID brings up additional details, including whether the EID has any flags, pending revisions or comments. Note that revisions can be pending for EIDs that are in both the Submitted/Unreviewed Status (yellow) and the Accepted Status (green). In other words, even once accepted, evidence may still be improved further.
General Evidence Item Curation Practices¶
Evidence Items should generally be prepared from primary literature rather than from review articles. It is recommended that curators use reviews to identify potential primary literature referenced in the review and to curate individual Evidence Items based on these cited articles. Review articles can also be used to develop Gene and Variant summaries. Similarly, evidence should not be created from introduction or discussion content in articles that are just restating previous findings of other works. Instead the curator should always try to find the primary/original source of information.
When curating new evidence, the curator should review the existing evidence already curated into CIViC for that Variant to look for the following issues:
For clinical trials and case reports (Levels A, B, and C), overlapping patient populations (i.e. the same patient treatment and outcome described in multiple reports) should be avoided, or carefully noted to alert users of this nuance and avoid conclusions that mistake these studies as independent. Note also that reports describing different phases of the same patient treatment (i.e. erlotinib and subsequently afatinib), or different clinically relevant conclusions (i.e. predictive evidence and simultaneous diagnostic evidence) are independent/non-overlapping entities.
For Predisposing EIDs, which generally describe germline molecular profiles (variants), the same patient may appear in multiple studies. Curators should be careful to note these cases and review existing germline EIDs for the same molecular profile in CIViC.
Disease stage, prior treatments, and other experimental details influencing evidence interpretation should be captured within the Evidence Statement to maximize user comprehension of the underlying study and the appropriate context in which it is relevant. Such details are critical parts of clinical guidelines and can impact which clinical guidelines should be used as well as interpretion of types of therapy response (see for example EID1008 and EID1009).
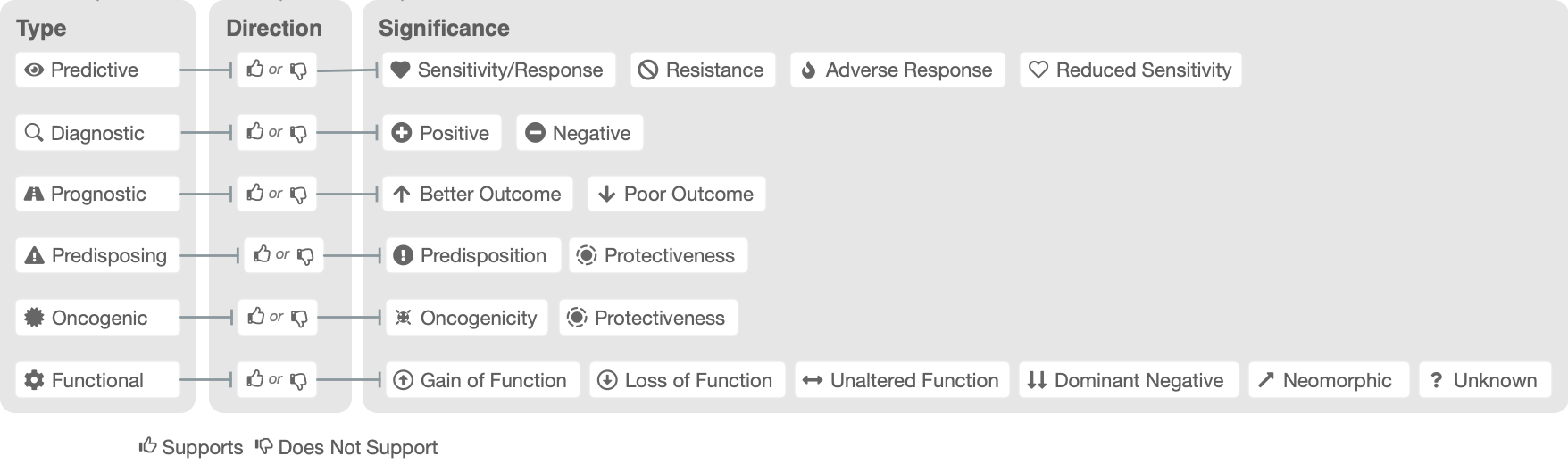
Six types of EID exist in CIViC (Figure 4), each giving structured clinical annotation to a Molecular Profile (Variant). Four types of clinical statements, Predictive/Therapeutic, Prognostic, Diagnostic and Oncogenic Evidence Types are usually associated with somatic molecular profiles (variants), while Predisposing evidence is generally linked to germline variation. Functional studies are often performed in vitro, so associated EIDs may often have the Unknown field selected for Molecular Profile (Variant) Origin.
Predictive Evidence¶
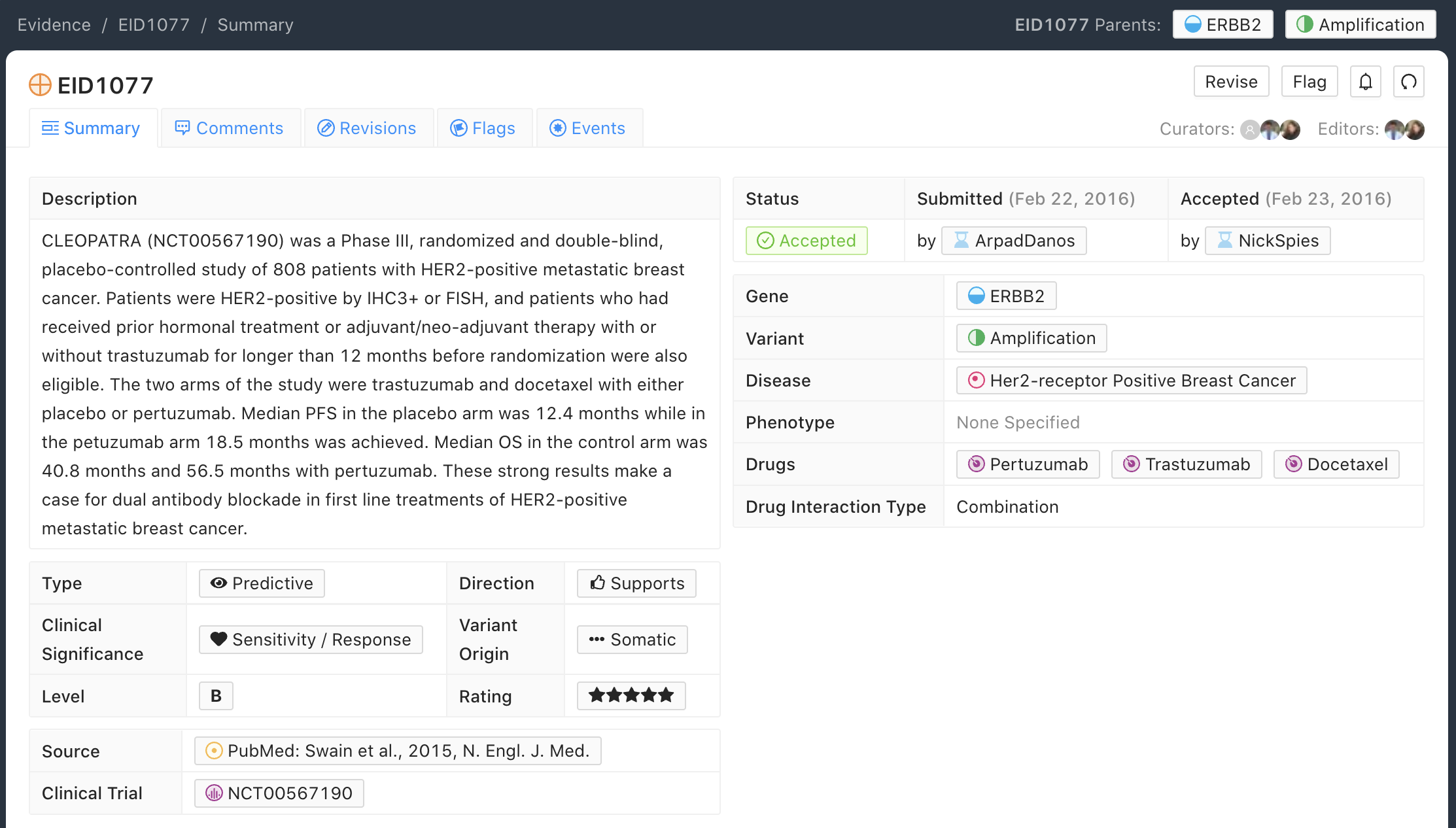
Predictive/Therapeutic Evidence Items (EIDs) capture evidence supporting or refuting the role of a molecular profile (variant) in conferring drug sensitivity, resistance or adverse response in the context of a specific disease.
Below is an example of an EID that illustrates the Predictive Evidence Type (Figure 5). This example describes the CLEOPATRA trial (NCT00567190), which evaluated 808 patients with HER2-positive metastatic breast cancer. These patients demonstrated significant sensitivity/response when treated with combination therapy of docetaxel, pertuzumab and trastuzumab.
Predictive Evidence Curation Practices¶
Predictive Evidence Items should include the Therapy (Drug) Name(s) and Therapy Interaction Type (for multiple therapies used in some kind of combination).
The most current name of the Drug (excluding trade names) should be used in the Therapy field to reduce duplication. The Evidence Statement should contain the therapy name used in the study with the current name in brackets, when applicable.
Therapy Interaction Types are required anytime more than one drug is mentioned for a given study. If multiple therapy interaction types are at play (e.g., combinations and substitutes), consider separating these concepts into more than one Evidence Item.
If applicable, the Clinical Trial name should be included in the Evidence Statement. Any clinical trial IDs available in PubMed for the Source linked to this Evidence Item will be automatically imported and linked to this Evidence Item when the PubMed Source is imported into CIViC.
The duration of exposure to the therapy and confounding interactions (e.g., wash-out periods, previous treatment, cancer stage) should be listed.
Assigning a Clinical Significance of Sensitivity/Response can depend on factors such as response rate, which will vary significantly with disease and treatment. In some cases a response rate of 15% may represent a significant improvement, and merit a classification of the Sensitivity/Response label. A general guideline for CIViC curation is to follow the author’s published (and peer-reviewed) interpretations and conclusions of the results.
Extensive guidelines, use cases, and examples for curation of predictive evidence are given in Figure 14 and Table 1.
Diagnostic Evidence¶
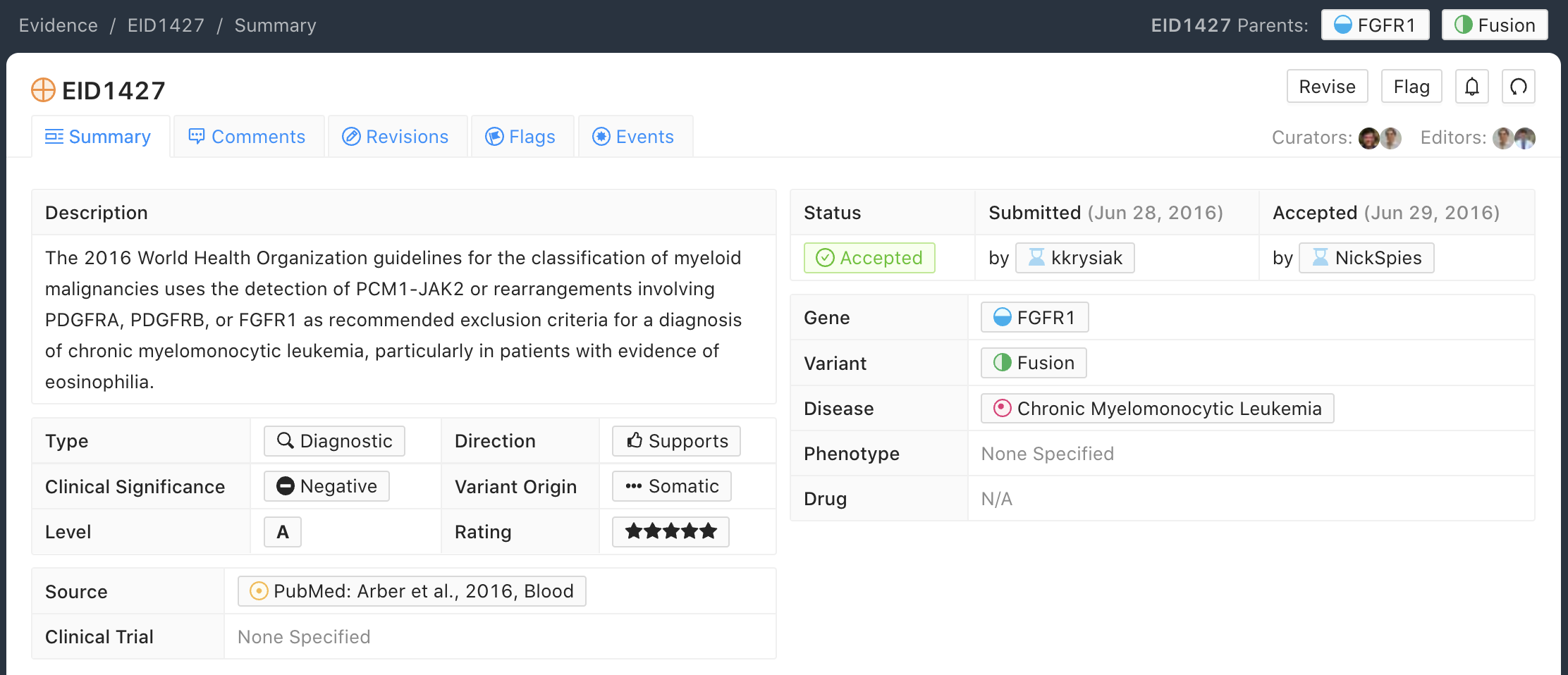
Below is an example of an EID that illustrates the Diagnostic Evidence Type. This example describes the World Health Organization guidelines for classifying chronic myelomonocytic leukemia (CMML). Specifically, if a patient has a PCM1-JAK2 fusion or a rearrangement involving PDGFRA, PDGFRB, or FGFR1, especially in the setting of eosinophilia, the patient does not have CMML.
Diagnostic Evidence Curation Practices¶
Diagnostic Evidence Items should only be used if the molecular profile (variant) assists in labeling the patient with a specific disease or disease subtype and should not be used to denote that the particular molecular profile is simply prevalent in a specific disease.
Generally, Diagnostic Evidence Items describe molecular profiles that can help accurately diagnose a cancer type or subtype with high sensitivity and specificity, for which diagnoses may otherwise be challenging.
Diagnostic Evidence Items should be very closely tied to the terms of the Disease Ontology (DO) in CIViC. The Disease Ontology works to actively generate mappings to other highly used ontologies, but the terms in the DO are generally accepted diseases which are part of medical practice. Therefore, literature proposing a novel disease type - for instance studies suggesting a novel cancer subtype defined by the presence of a specific oncogenic variant - are not generally admitted as part of the CIViC data model. Alternatively, if a curator with expertise in the field feels that the novel subtype has met with a sufficient level of acceptance, they may submit this type of Evidence Item using a non-DO term, and suggest that the DO admit this term into the ontology.
Literature describing diagnostic practice guidelines (such as those of the World Health Organization) may be used in curation and submitted as A-level Evidence Items.
Literature describing small numbers of observations in patient samples of a certain molecular profile (variant), where the authors state that the molecular profile may have diagnostic value, may be admitted as lower Evidence Rating (1-2 star), Case Study (C-level) data. Similar literature employing larger numbers could be labeled as Clinical (B-level).
Guidelines and use cases for curation of diagnostic evidence are given in Table 1.
Prognostic Evidence¶
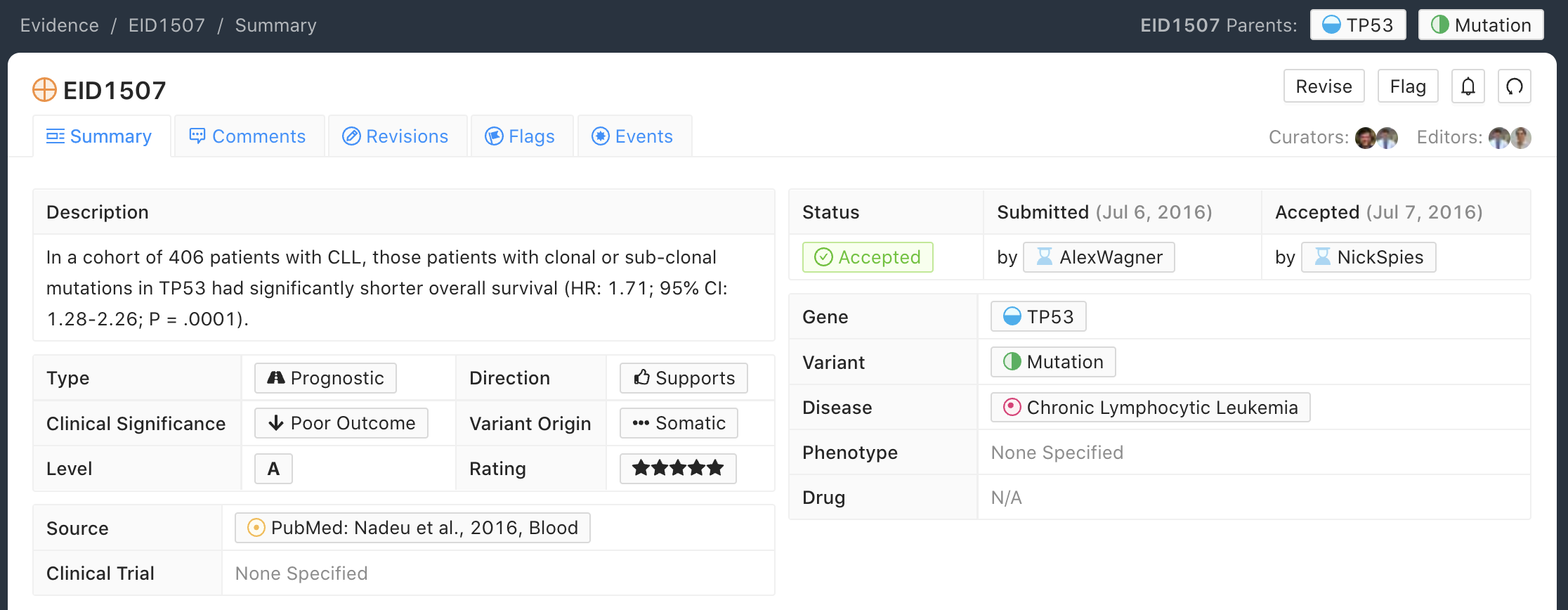
Below is an example of an Evidence Item that describes a Prognostic Evidence Type. This example describes a 406-patient trial whereby observation of any somatic TP53 mutation in chronic lymphoblastic leukemia conferred poor prognosis relative to wildtype TP53.
Prognostic Evidence Curation Practices¶
Prognostic Evidence Items should include the measured outcome (e.g., overall survival, complete response, partial response), number of subjects and applicable statistics.
If described in the literature, a definition of the measured outcome should be given.
Prognostic evidence is characterized by either better outcomes for patient subpopulations with the given molecular profile (variant), which are not specific to any particular treatment context, or worse outcomes which are not indicative of resistance to a specific treatment. Instead, the change in outcome should be largely correlated to the presence of the molecular profile.
In some cases, a molecular profile (variant) subpopulation with worse outcome may benefit from subsequent therapy targeted to that molecular profile (e.g., HER2 amplification in breast cancer).
Guidelines, use cases, and examples for curation of prognostic evidence are given in Figure 14 and Table 1.
Predisposing Evidence¶
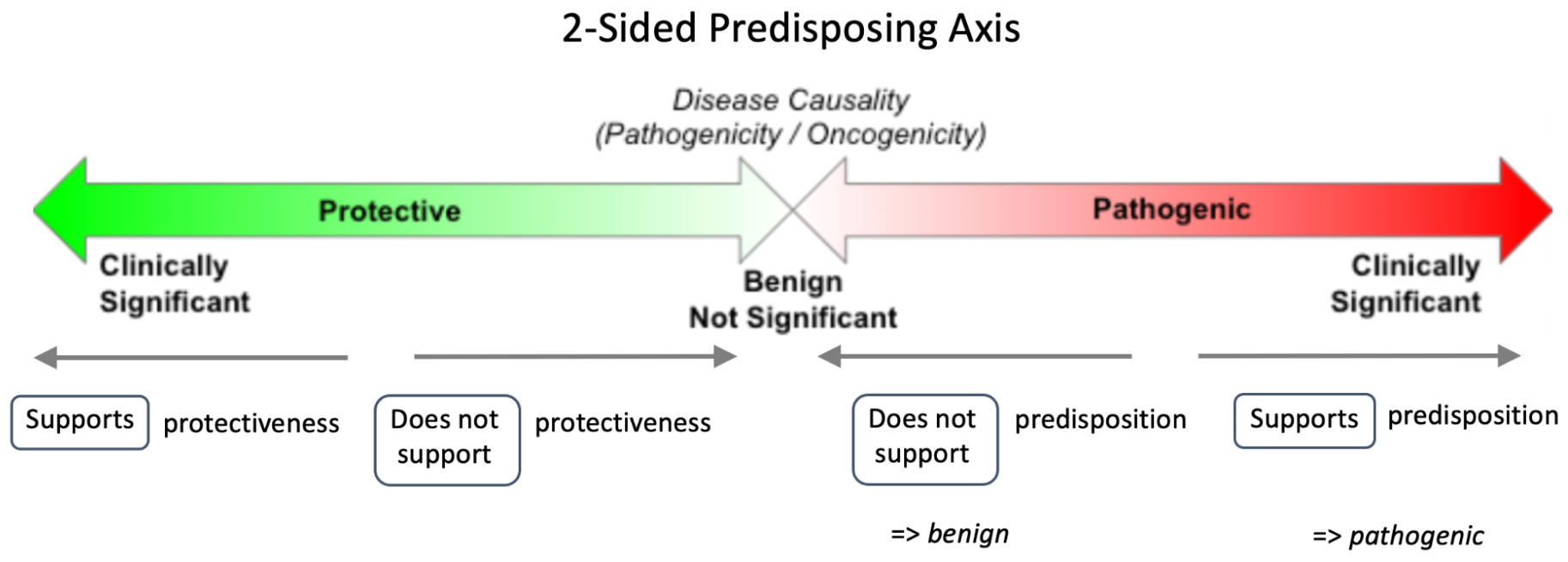
Predisposing Evidence Items were first introduced in CIViC v1 to capture the role of a molecular profile (variant) in increasing the likelihood of developing cancer. This is comparable to the concept of heritable genomic variants that increase risk for “cancer predisposition syndromes” or “cancer susceptibility”. In CIViC v2, Predisposing Evidence Items include both this historical clinical significance of “cancer predisposition variants”, as well as evidence items that decrease risk for cancer susceptibility by conferring a protective effect (“cancer protectiveness variants”). The structure of Predisposing Evidence Items (EIDs) mirrors the structure of other EID types in CIViC by having multiple clinical significance classifications under which evidence can be evaluated. (Figure 8). Thus, just as Prognostic EIDs capture better and worse outcomes, and Predictive EIDs include the ability to capture sensitivity and resistance, the Predisposing EID can capture detrimental pathogenic and also beneficial protective qualities. CIViC Predisposing Evidence Items which pertain to the Pathogenic axis in Figure 8 can be aggregated at the CIViC Assertion level for a formal pathogenicity evaluation utilizing ACMG/AMP Codes.
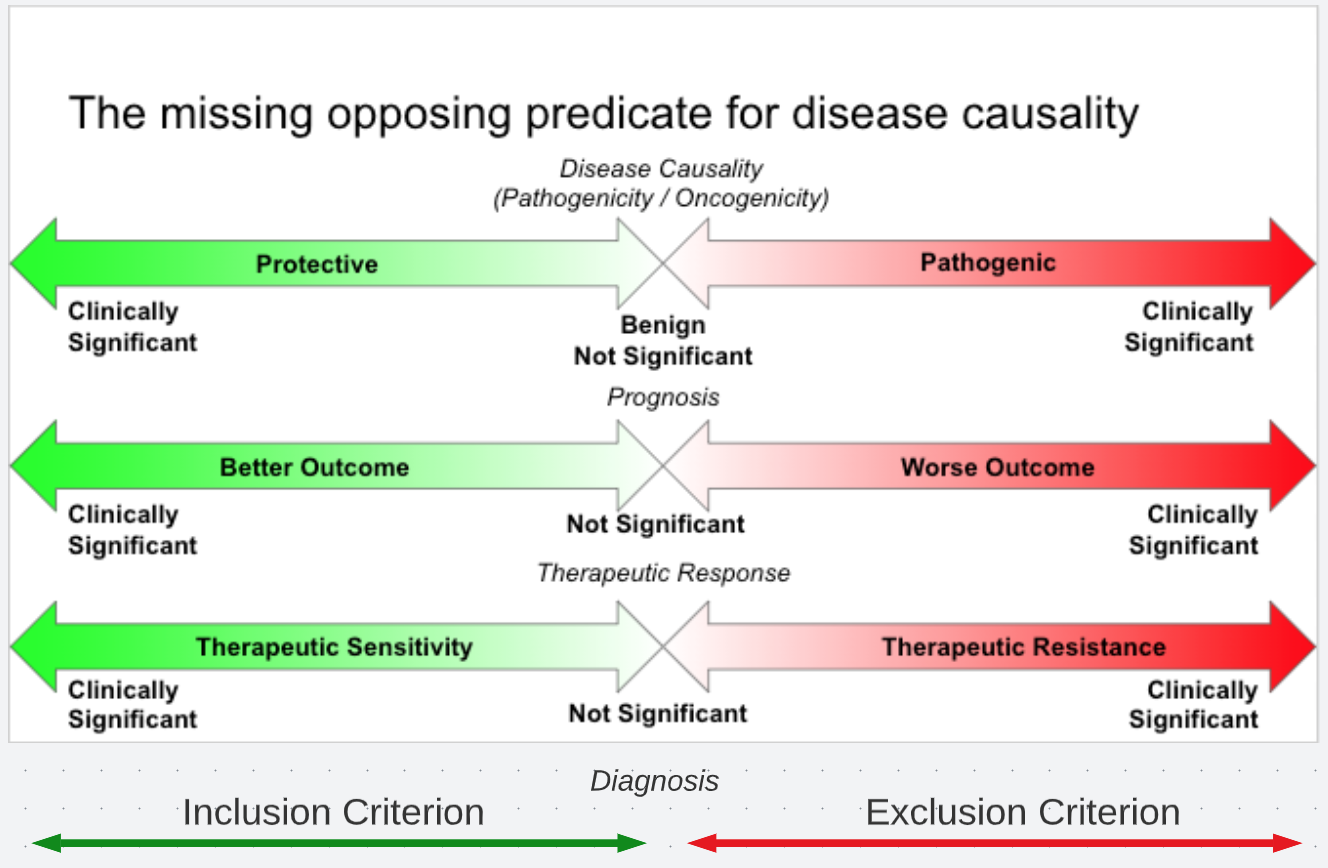
The Pathogenic axis for Predisposing EIDs (right side in Figure 8) documents evidence which describes either the presence or absence of a pathogenic property for a molecular profile (variant). It is important to realize that evidence supporting both a pathogenic or benign classification are captured using the Predisposition clinical significance, associated with the right (red) axis (labeled Pathogenic) by use of the CIViC Evidence Direction (Supports or Does not support) (Figure 9). To summarize, a CIViC Predisposing EID that Supports clinical significance of Predisposition suggests a potentially pathogenic molecular profile (variant). A Predisposing EID that Does Not Support clinical significance of Predisposition suggests a potentially benign molecular profile (variant). These EIDs do not make any final classification of pathogenicity and may or may not fully support any specific ACMG criteria but point in the direction of such classifications.
As mentioned above, the Predisposing Evidence Type may utilize ACMG/AMP Codes when applicable. If the curator wishes to capture evidence that indicates a molecular profile (variant) may be benign or pathogenic, and this evidence meets one or more of the published criteria from ACMG/AMP guidelines (termed ACMG codes in CIViC), then the curator can indicate the ACMG codes that were met in the body of the EID. The general format for a predisposing EID of this type is a summary of the reported data relevant to the molecular profile (variant) and disease of interest, followed by an enumeration of ACMG Code(s) derived from the reported information with a brief justification for the presence of each code.
Note that currently, ACMG/AMP criteria should be restricted to simple (single variant) Molecular Profiles. Multiple ACMG criteria are not forumlated for groups of co-occuring variants accross different genes. For example PM1 (Located in a mutational hot spot and/or critical and well-established functional domain) is not clear wether this would be required of one or all of the variant members of a complex MP. PP1 (Cosegregation with disease in multiple affected family members in a gene definitively known to cause the disease) is also clearly not defined for combinations of varinats.
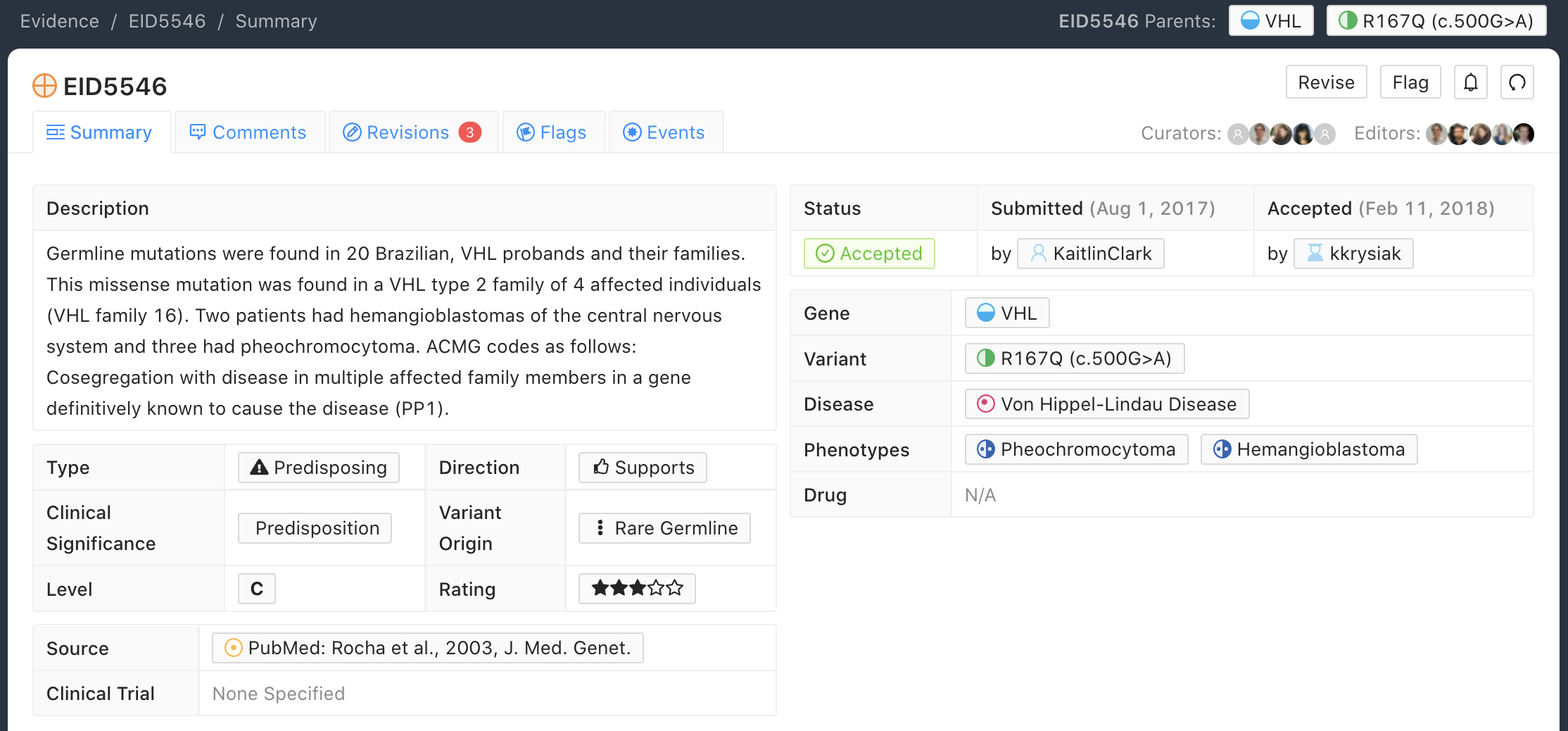
Below is an example of an Evidence Item (EID5546) that describes a Predisposing Evidence Type (Figure 10) that Supports a Significance of Predisposition. This example describes a study where the VHL - R167Q (c.500G>A) Variant was described in a set of patients and evidence for the PP1 ACMG-AMP criteria was documented. Hemangioblastoma and pheochromocytoma were seen in patients and are reported as Associated Phenotypes, while the Disease is Von Hippel-Lindau Disease.
Predisposing Evidence Curation Practices¶
Typically, but not always, Predisposing Evidence Items are written for rare germline variants. In rare circumstances, the patient can have a predisposing variant that develops as a result of a somatic mutation or mosaicism during embryogenesis that is widespread, but not necessarily heritable. Common germline variants may also be associated with predisposition to cancer.
For evidence that indicates the presence or lack of a protective quality for a germline molecular profile (variant), this will be annotated with Supports Protectiveness or Does not support Protectiveness, respectively. Although not yet well-described in cancer predisposition, we anticipate examples will become available with time based on other complex diseases, such as the APOE2 allele which has evidence that it is protective against Alzheimer’s disease.
Evidence supporting pathogenicity will be captured by a curator by selecting Supports, and then Predisposition using the menus available on the Add Evidence form in CIViC. Importantly, evidence supporting a benign annotation will be captured during curation by choosing Does Not Support and then Predisposition in the menus available in the Add Evidence form.
For EIDs that utilize the Significance value Predisposition, ACMG evidence criteria (Richards et al 2015) (termed ACMG codes for short) are derived from the evidence presented in the specific Evidence Source and are listed at the end of the Evidence Statement with a brief justification for each code’s use. ACMG evidence codes that can not be directly derived from the Evidence Source (e.g., population databases for PM2) should be captured in the Molecular Profile Description or at the level of the Assertion. The EID depicted here is part of Assertion number 4 (AID4), where the Evidence Items combine to create a Pathogenic Assertion. Predisposing Evidence Items do not individually determine ACMG/AMP Pathogenicity, but simply show in which direction the evidence derived from the particular publication or abstract is “leaning”, e.g., if it is leaning towards a pathogenic or benign final classification.
Oncogenic Evidence Type¶
Oncogenic Evidence Items (EIDs) capture clinically relevant information associated with either a somatic molecular profile’s (variant’s) protective qualities or, more commonly, its involvement in tumor pathogenesis as described by the Hallmarks of Cancer. An Evidence Statement for an Oncogenic EID includes a summary of the reported data relevant to the molecular profile and disease of interest by describing assays performed and experimental results. The Evidence Summary for an Oncogenic EID may contain Oncogenicity Codes from the ClinGen/CGC/VICC Standards for the classification of oncogenicity of somatic variants in cancer.
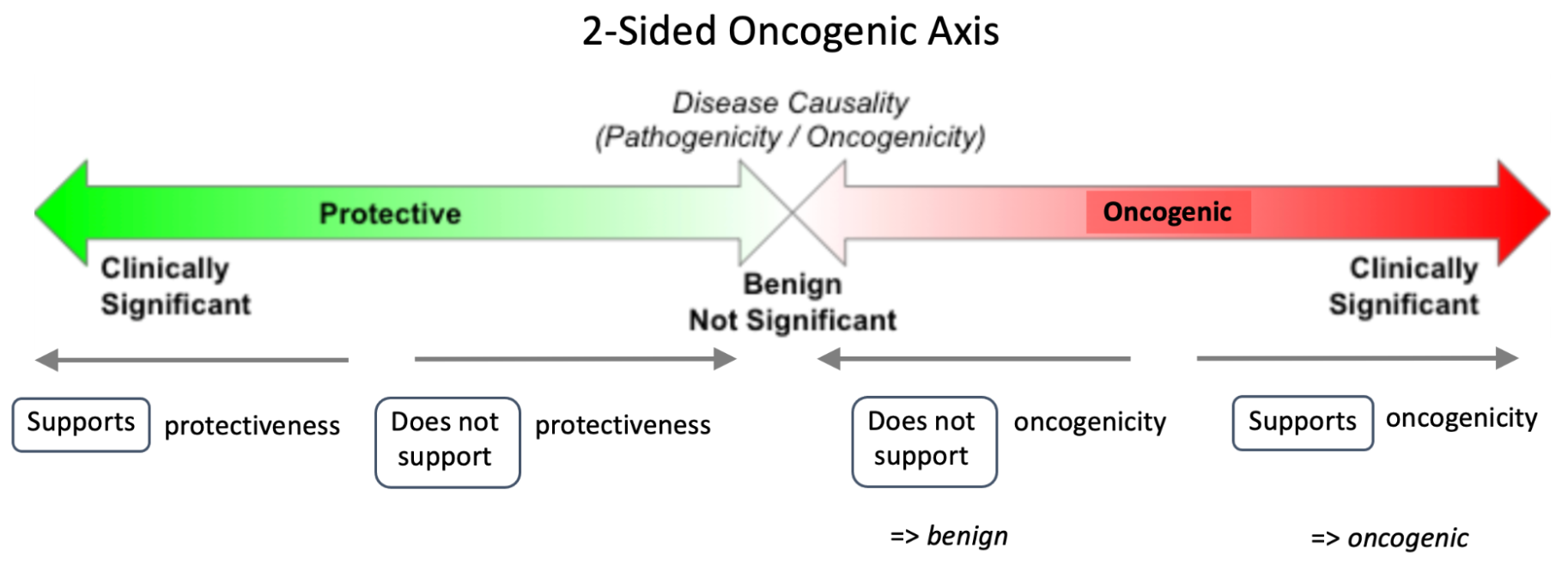
In a system similar to the one described above for Predisposing Evidence Items, the Protective Clinical Significance may be used to capture evidence associated with a somatic variant’s ability to reduce the development or harmful effects of a tumor. For example, the association of enhanced DNA-damage repair with significant TP53 copy number gains (PMID: 27642012).
The Oncogenic Clinical Significance is used to capture evidence supporting an oncogenic or benign final classification of a somatic molecular profile (variant) at the Assertion level. In the case where evidence suggests a Molecular Profile has oncogenic properties, a curator will select Supports, and then Oncogenicity using the menus available on the Add Evidence form in CIViC (Figure 11). Importantly, evidence supporting a benign annotation will be captured during curation by choosing Does not support and then Oncogenicity in the menus available in the Add Evidence form.
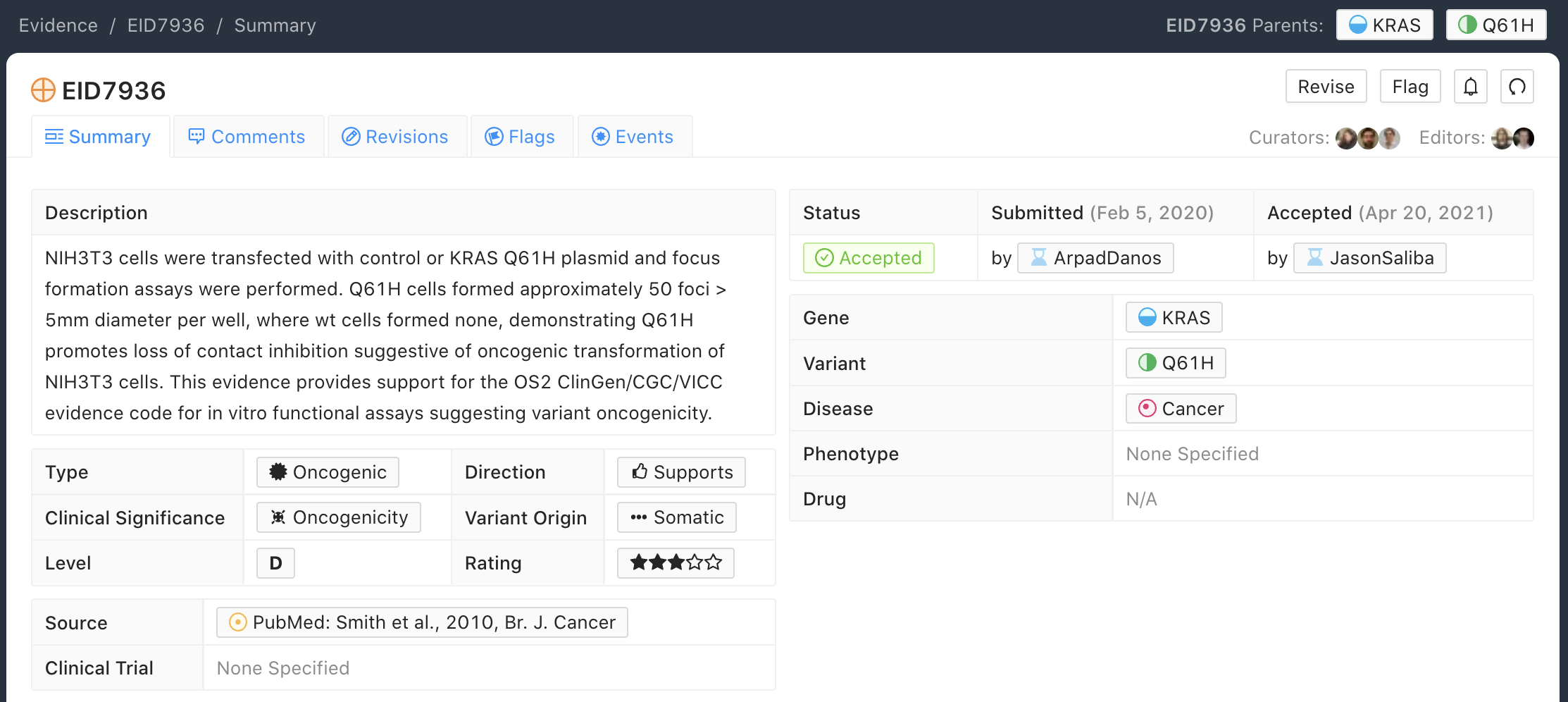
Below is an example of an Evidence Item with an Oncogenic Evidence Type (Figure 12). This EID describes a study wherein KRAS Q61H was transfected into cells resulting in multilayered growth indicative of a loss of contact inhibition. Oncogenicity code OS2 is noted in the Evidence Statement, since the EID describes a well established in vitro experiment (focus formation assay), which supports an oncogenic effect for this variant.
Oncogenic Evidence Curation Practices¶
The Oncogenic Evidence Type describes literature-derived evidence pertaining either to a somatic molecular profile’s (variant’s) protective effects or its role in tumor formation, growth, survival or metastasis, as summarized by Hanahan and Weinberg in Hallmarks of Cancer. Disease type should be specified, as oncogenic effects may depend on cellular context (expression of a gene in a given tissue type, activity of the relevant pathway, etc.). For cases where a disease type is difficult to ascertain, such as experiments in highly de-differentiated cell lines, the Disease Ontology term ‘Cancer’ can be used. The Evidence Statement should contain a summary of the experiments or findings suggesting a protective, oncogenic, or benign effect.
The Oncogenic Evidence Item may be associated with Oncogenicity Codes developed by the Knowledge Curation and Interpretation Standards (KCIS) working group of the GA4GH VICC in collaboration with ClinGen working groups and Cancer Genomics Consortium (CGC) Oncogenicity codes assess oncogenicity of a given somatic variant in a mechanism similar to that used in the 2015 ACMG/AMP Guidelines for germline pathogenicity. Enumeration of Oncogenicity Codes derived from the literature along with a brief justification for the assignment of each code can be included in the Evidence Statement.
Currently application of ClinGen/CGC/VICC guidelines is restricte to Evidence Items associated to simple Molecular Profiles (MPs) which consist of only one variant. Complex MPs comprising more than one variant are out of the guideline scope. For example criteria utilizing cancerhotspots or COSMIC data are not well defined for co-occurring variants, as the variant frequencies are only reported for variants in isolation.
Functional Evidence Type¶
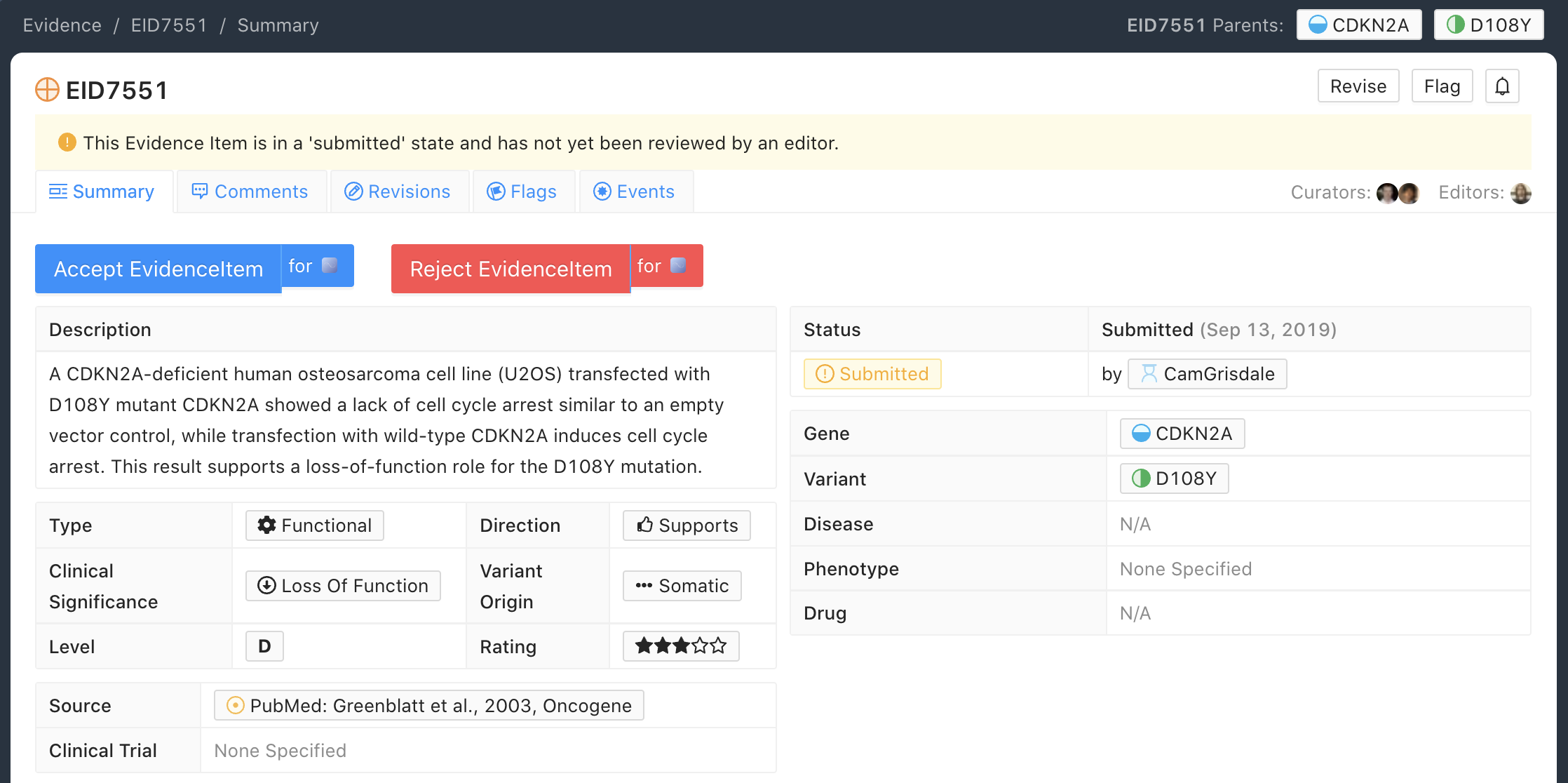
The Functional Evidence Type describes data from in vivo or in vitro experiments that assess the impact of a molecular profile (variant) at the protein level (often can be thought of a biochemical effect). Functional Evidence should be disease agnostic and if the Evidence being entered relies on disease or cell context, consider another Evidence Type. The Molecular Profile (variant) Origin for this Evidence Type is anticipated to primarily be N/A and entries should be classified under the Evidence Level of D - Preclinical. Variant impact on protein structure, folding, binding, activity, activation, phosphorylation, protein-protein interaction, sub-cellular localizatoin, and downstream pathway signaling are all examples of types of evidence that fall under the Functional Evidence Type. For variants in functional non-coding, impact might relate to things like RNA stability, folding, recognition of binding targets, etc.
Below is an example of a Evidence Item that describes a Functional Evidence Type (Figure 13). The authors performed an experiment to determine the impact of the variant on normal protein function related to cell cycle arrest. Expression of wildtype CDKN2A arrests the cell cycle in CDKN2A deficient cells, whereas expression of CDKN2A D108Y does not impact cell cycle progression in the CDKN2A deficient cells. These results indicate the innate ability of CDKN2A to arrest cell cycle progression has been lost as a result of the presence of the protein variant.
Functional Evidence Curation Practices¶
Functional Evidence Items describe how the molecular profile (variant) alters (or does not alter) biological function from the reference state. The Evidence Statement should include details on the experimental conditions (e.g., specification of cell type and/or model system, expression vector, vector entry system, and selection method) and the results related to the potential impact on function (including statistics, if applicable).
Significance for Functional Evidence Types adhere to the following rules related to Muller’s Morphs:
Gain of Function |
A variant whereby enchanced/increased level of function is conferred on the gene product |
Loss of Function |
A variant whereby the gene product has diminished or abolished function |
Unaltered Function |
A variant whereby the function of the gene product is unchanged |
Neomorphic |
A variant whereby the function of the gene product is a new function relative to the wildtype function |
Dominant Negative |
A variant whereby the function of a wildtype allele gene product is abrogated by the gene product of the allele with the variant |
Unknown |
A variant that cannot be precisely defined by gain-of-function, loss-of-function, or unaltered function. |
Functional Evidence Items may be used to support certain ACMG or Oncogenicity codes (e.g. PS3 or OS2 respectively). In these cases, the ACMG or Oncogenicity code should be listed in the Evidence Statement along with a brief justification for its inclusion. Functional Evidence Items may appear as supporting evidence for Predisposing or Oncogenic Assertions.
Curation Scenarios¶
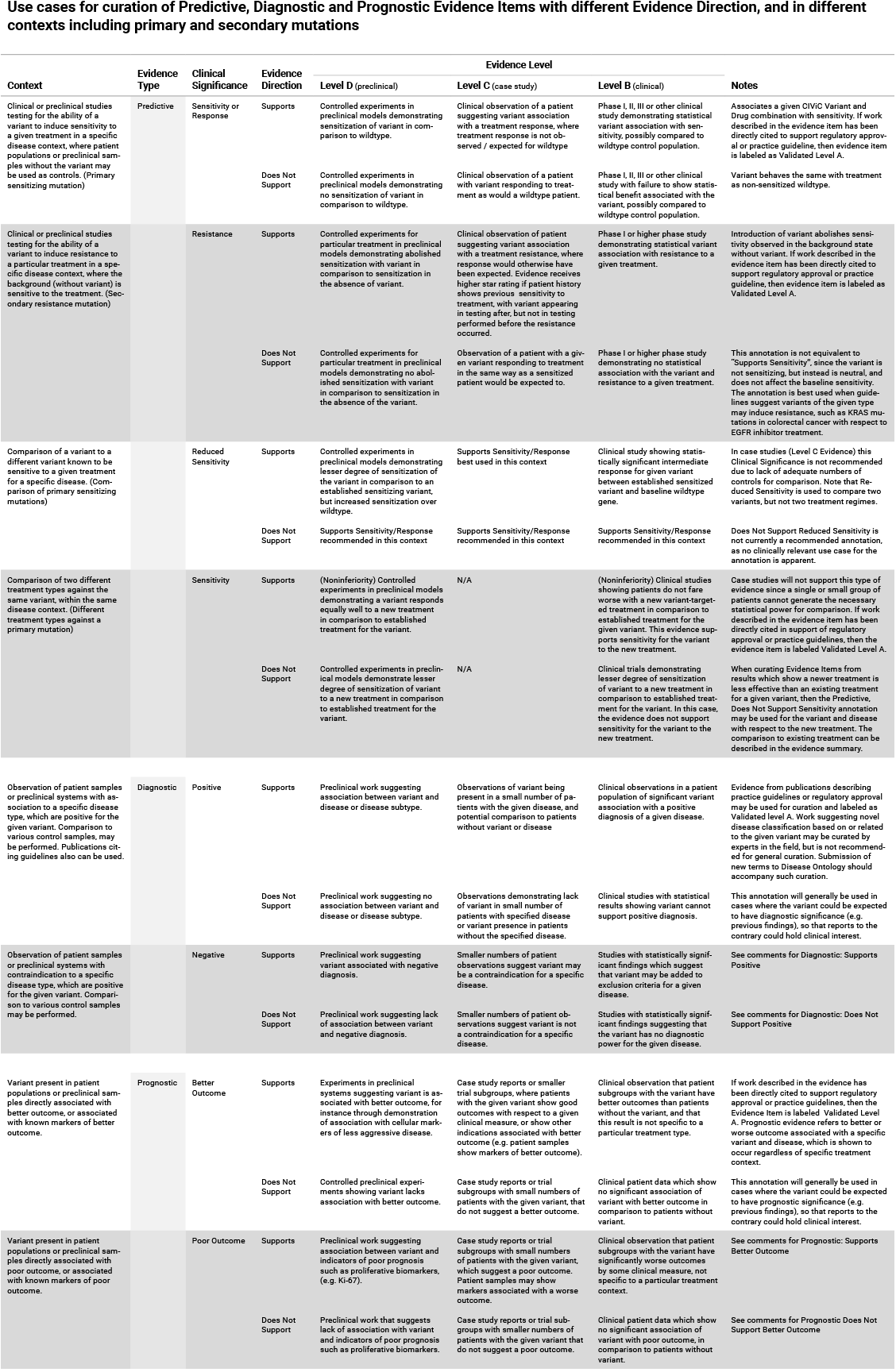
The table below (Table 1) gives an in depth set of cases for assigning the Significance to an Evidence Item (EID) where either the “Supports” or “Does Not Support” Evidence Direction is used in combination with a Predictive/Therapeutic, Diagnostic or Prognostic Clinical Significance annotation.
Note that “Reduced Sensitivity” Clinical Significance is used to compare the molecular profile (variant) of interest to a known, sensitizing molecular profile. It is not used to compare the efficacy of one drug for a molecular profile against a different drug for the same molecular profile. In the latter case, the curator may simply make a Predictive evidence item which independently evaluates the efficacy of the drug against the molecular profile of interest.
The “Sensitivity/Response” annotation is used to assess sensitizing molecular profiles (variants), which are usually in the form of a primary sensitizing somatic mutation (e.g SNV, amplification, deletion, etc).
The “Resistance” annotation is used in situations where the molecular profile (variant) of interest has been observed to induce resistance in a context where, in the absence of the molecular profile, the system being assayed would be deemed sensitive which induce resistance to treatment (e.g. T790M mutation in cis with a background variant of EGFR L858R). In cases where a variant fails to induce sensitivity, then that molecular profile is best annotated with “Does not Support Sensitivity”.
A more readable version of Table 1 can be downloaded as a PDF here
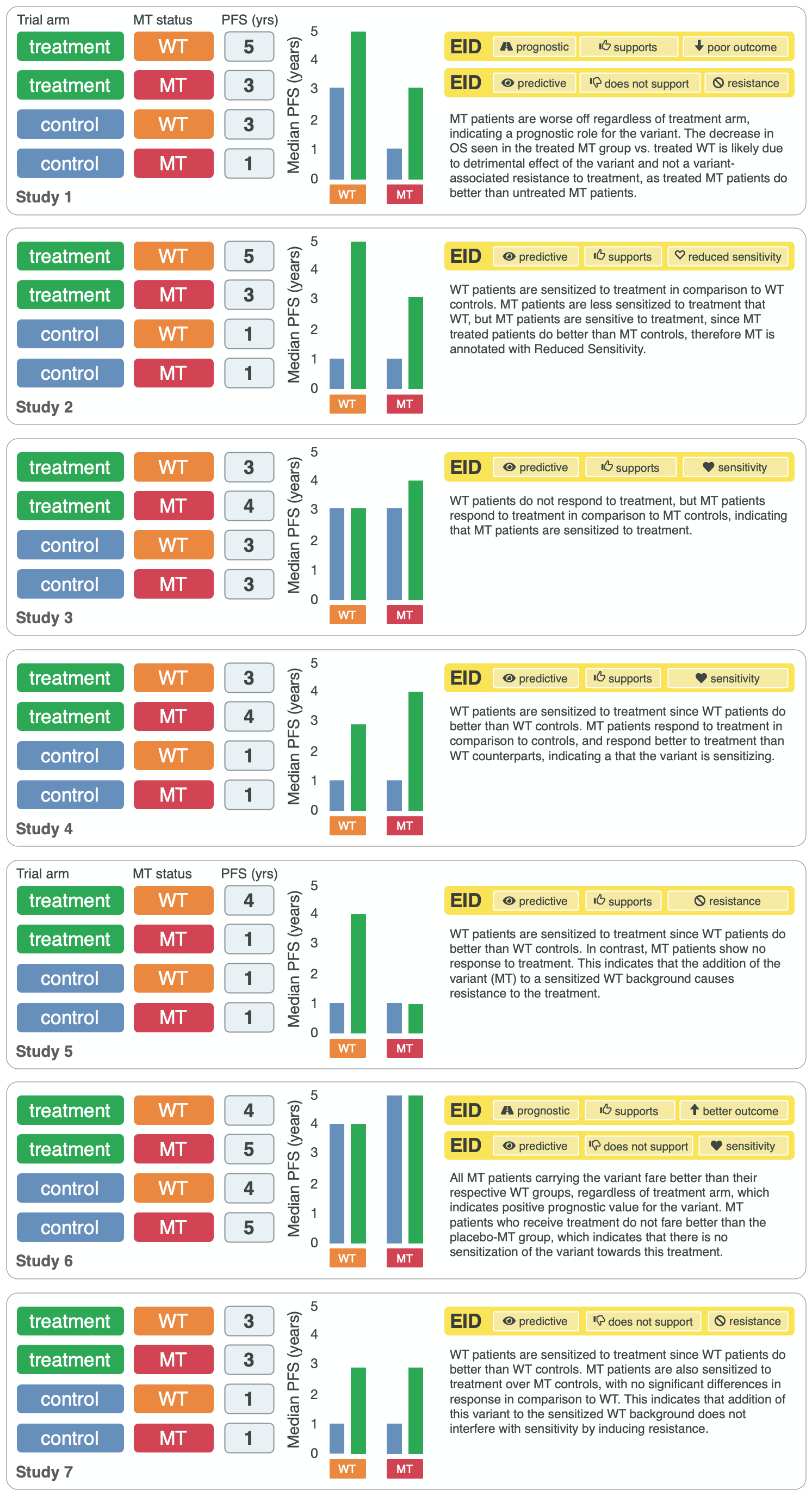
Both Predictive and Prognostic evidence types may be obtained from the same data set in some cases. Figure 14, displayed below, gives hypothetical examples of predictive and prognostic structured annotation derived from patient data.
Curating Evidence from Clinical Trials¶
When curating evidence obtained from clinical trials performed with groups of patients, where data is pooled by mutation type (e.g. EGFR MUTATION), Level B clinical results may be obtained, which may report a statistically significant difference on a clinically relevant parameter such as partial response (PR) between wildtype vs. mutant patients. In addition, the publication may sometimes give outcomes on important individual patient parameters, such as variant, age, sex, best response, overall survival, etc. In these cases, this aggregate of data may be integrated into multiple Evidence Items in the following manner (The figure below is loosely based on a data set in CIViC obtained from PMID:21531810, which can be seen in CIViC on its Evidence Source page).
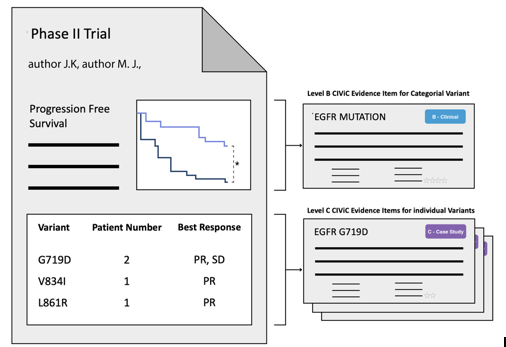
Statistical results may be obtained from the study to annotate a Categorical (sometimes colloquially called bucket) CIViC Molecular Profile (Variant), which pools together a category of sequence variants (for example EGFR MUTATION). Significantly longer progression free survival (PFS) may be observed in the mutant group (grouped under the Categorical CIViC Variant) vs. the wildtype group, when given a certain drug. In this case, this result may be reported in a CIViC Level B Evidence Item under the CIViC Categorical Variant EGFR MUTATION, with Evidence Direction and Clinical Significance “Suggests Sensitivity/Response” to the drug used.
When a sufficient level of individual patient detail is present, including the individual patient variants along with an important clinical parameter such as their best response, then this data set can be used to generate a set of CIViC Level C Evidence Items for the patients, each one associated with the respective CIViC Variant that was observed in the individual patient, along with the outcome. Note that even if the entire group showed statistically significant improvement with the Categorial Variant, this does not mean every patient did better, e.g. if a patient with variant X123Y had progressive disease as best response, then this would result in a Level C EID with Evidence Direction and Clinical Significane of “Does not support Sensitivity” for the CIViC Variant X123Y.
Complex Molecular Profiles in comparison to Categorical (Bucket) MPs¶
In the above examples, the Bucket MP EGFR Mutation is utilized. Other examples of Categorical (Bucket) MPs are ALK Fusion, or BRAF Amplification. These MP types create a category for, or bucket together a set of variants that is not simply enumerable, since there are in principle an unrestricted number of ways a variant can meet the criteria to be part of the bucket MP. In contrast, an MP such as BRAF V600E OR BRAF V600K can be easily enumerated as a complex MP of two elements. A more nuanced case could be the MP BRAF V600, which allows for any amino acid to occur at this position. While this can be enumerated with a 20 element complex MP, that would clearly be difficult to accommodate with the CIViC user interface, and also would not reflect the shorthand used by the field. Therefore, in cases like this, it is recommended to utilize the compact categorical MP notation, in this case BRAF V600.